
In 2025, U.S. healthcare organizations reported 642 large data breaches affecting 57 million people , and a single breach in the sector still costs an average of USD 7.42 million according to Chief Healthcare Executive, the highest of any industry for the 14th year running. Most of those incidents trace back to software: misconfigured servers, weak access controls, broken APIs, untested AI components.
This is why healthcare application testing becomes the line between a working clinic and a breach disclosure. A bug in your fintech app costs a refund. A bug in an EHR or remote monitoring platform can mean a missed dose, a leaked diagnosis, or a class-action lawsuit.
We at Binariks treat it accordingly: every healthcare project goes through compliance-driven validation under our QA & testing services .
After reading this article, you will know:
- How healthcare testing differs from standard QA, and why that gap costs millions when ignored
- Which regulations (HIPAA, FDA 21 CFR Part 11, IEC 62304, ONC) shape your test strategy in 2026
- How to validate AI/ML components, including LLM-based test generation and SaMD-specific scenarios
- What it actually costs, who needs to be on the QA team, and where most testing programs break down
The next ten minutes will save you from a six-figure compliance bill. Let's get into it.
What is healthcare application testing?
Healthcare application testing is the validation discipline that proves clinical software works as intended, protects patient data, and survives a regulatory audit. The bar is rising.
In its September 2025 final guidance on Computer Software Assurance, the FDA stated that "software testing alone is often insufficient to establish confidence that the software is fit for its intended use", and pushed manufacturers toward a continuous, risk-based assurance model. Translation: shipping a passing test suite no longer counts as "validated".
That shift matters because it separates software testing in healthcare from QA in any other vertical. A standard web app gets tested for functionality, performance, and a baseline of security. A healthcare app gets tested for all that plus interoperability with HL7 and FHIR, audit trails that satisfy FDA rules, encryption that holds under HIPAA, and clinical accuracy validated against real-world patient scenarios.
Quality assurance in healthcare is not a quality function bolted onto engineering. It is a regulatory-grade evidence pipeline that runs the entire product lifecycle.
E-commerce vs. Healthcare: the clear difference
| Bug type | E-commerce impact | Healthcare impact |
| Form validation breaks | Cart abandoned, refund issued | Wrong dosage entered into EHR |
| API timeout | Order delayed | Lab result not returned to clinician |
| Auth bypass | Stolen credit card | PHI breach, OCR fine, class-action lawsuit |
| Data field mismapping | Wrong shipping address | Wrong patient flagged for surgery |
The e-commerce column ends in customer service tickets. The healthcare column ends in patient harm, regulatory penalties, and headlines.
We saw this firsthand on an AI-powered cardiac screening platform , where the same model behavior that would be a "minor accuracy issue" in a recommendation engine had to be validated across more than 30 European clinical centers before deployment.
There is no margin for "good enough" when the output drives a diagnosis.
Why healthcare application testing matters: Regulatory and safety context
The case for medical software testing is not abstract. It splits into three concrete categories of risk: people get hurt, regulators show up, and your business takes a hit it may never fully recover from. Skip rigorous QA on a clinical product, and at least one of these three lands on your desk within 18 months. Often all three.
Patient safety risks
The 2025 Ponemon Institute study found that 72% of U.S. healthcare organizations hit by cyberattacks suffered patient care disruption, and 29% of those reported "patient mortality rates increased".
A medication-dosing module that miscalculates because a unit conversion was never tested. An EHR that drops a critical allergy flag during a sync with a third-party lab. An infusion pump UI that freezes mid-titration. These are the bugs an unbothered QA team ships and a coroner later finds.
Regulatory compliance obligations
If patient harm does not concentrate the mind, the regulatory pile-up will. A 2026 healthcare app has to pass review under HIPAA for data protection, FDA rules for electronic records and audit trails, the international standard for medical software lifecycles, and ONC certification for any system that exchanges patient data.
Outside the U.S., add EU medical device rules, GDPR, and standards for standalone health software. Each framework demands its own evidence trail: traceability matrices, risk analyses, validation reports, audit logs that survive a subpoena. OCR's 2025 enforcement initiative made the cost of getting this wrong unmistakable.
Business and reputational risk
The IBM Cost of a Data Breach figures we cited earlier ($7.42M average per healthcare breach) only capture direct financial impact. They do not include the class-action lawsuits that now follow virtually every PHI exposure, the OCR corrective action plans that lock organizations into three-year compliance monitoring, or the customer churn when a hospital network publicly disengages.
There is also the recruitment problem that hits engineering once a breach makes the news. We have seen this calculus play out across our healthcare software development services : the clients who treated QA as a cost center paid the bill in litigation.
Healthcare software testing sits at the intersection of clinical safety, regulatory exposure, and business survival, and the 2025 numbers prove that all three risks are now actively materializing.
Types of healthcare application testing
Generic QA frameworks split testing into a tidy taxonomy: functional, non-functional, regression, the usual. Healthcare breaks that taxonomy. The mix shifts because the consequences shift, and a 2026 testing programme has to cover seven distinct disciplines, each with its own evidence trail. Skip one, and the gap shows up in an audit, a breach disclosure, or a clinician complaint.
Functional testing
Functional testing verifies that each feature does what the requirements say it should do, end to end. In a healthcare context, "feature" means an appointment scheduler that books across time zones without double-booking, a prescription module that calculates dosing by weight without rounding errors, a billing engine that maps procedure codes correctly.
Testers walk through every clinical workflow with positive and negative cases, including edge inputs that real patients actually generate (impossible birth dates, allergy lists with 40+ entries, names with diacritics).
Why it matters: in e-commerce, a failed checkout means a lost sale. In a hospital, a failed medication-order workflow means a patient gets the wrong drug. The 2024 Ponemon Institute data we cited earlier showed that 54% of breached organizations linked attacks to "increased medical procedure complications", and a meaningful share of those start as undetected functional defects, not exotic exploits.
Security and compliance testing
This combines penetration testing, vulnerability scanning, encryption validation, access-control verification, and audit-trail proof. The tester's job is to behave like an attacker, then like an auditor.
What gets checked: PHI encryption at rest and in transit, role-based access controls with documented minimum-necessary access, session-management against token replay, breach-detection logging that survives a regulator's subpoena.
Interoperability and integration testing
Interoperability testing validates that the application speaks every required standard correctly: HL7 message parsing, FHIR resource handling, DICOM for medical imaging, X12 for claims. What gets checked: schema conformance, terminology mapping (ICD-10, SNOMED CT, LOINC), latency under realistic message volumes, error handling when a downstream system returns malformed data.
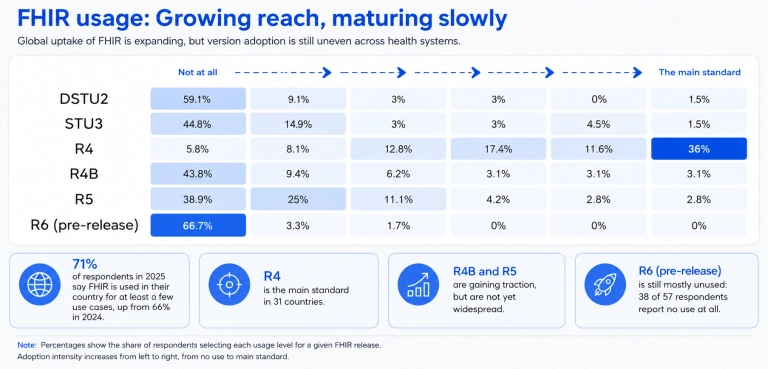
The HL7 International 2025 State of FHIR survey found that fragmented and inconsistent implementation across vendors remains one of the largest blockers to adoption.
We have walked clients through this exact problem on multiple engagements covered in our FHIR integration guidance , where the testing surface is bigger than the build surface. Get the integration tests wrong and your "interoperable" platform silently corrupts patient records every time a partner system updates its API.
Performance and load testing
Performance testing measures how the application behaves under stress: response times, throughput, resource utilization, graceful degradation under load. Performance testing for healthcare applications has stricter pass criteria than most industries because the user is a clinician with a patient on the table.
What gets checked: page-load times under peak hospital census, API response times during shift change when 500 nurses log in simultaneously, database query performance when an EHR fetches a 20-year patient history, failover behavior when a node drops.
Why it matters in healthcare specifically: a 4-second delay on an Amazon page costs a sale. A 4-second delay on a clinician's chart view during a code blue costs minutes that don't exist.
UI/UX and accessibility testing
UI/UX testing validates that real users, including clinicians wearing gloves, elderly patients with low vision, and screen-reader users, can complete tasks without errors or workarounds.
Accessibility testing specifically validates against the Web Content Accessibility Guidelines at level AA. What gets checked: keyboard-only navigation, screen-reader compatibility, color contrast for clinical alerts, touch-target size for tablet-based EHRs, cognitive load on emergency screens.
This stopped being optional in 2024. The HHS Section 504 final rule requires every healthcare website, mobile app, and patient-facing kiosk receiving federal funding to meet WCAG 2.1 Level AA, with enforcement starting May 2026. Non-compliant organizations face OCR action, ADA lawsuits, and lost contracts.
Medical device and IoT testing
Connected medical devices, infusion pumps, glucose monitors, pacemakers, hospital wearables, and the apps that control them require their own testing discipline. Clinical software testing for these devices includes hardware-software integration, firmware update verification, signal-acquisition accuracy, low-power behavior, and resilience to wireless interference.
What gets checked: data accuracy across temperature ranges, behavior under battery drain, security of the wireless protocol (Bluetooth LE, Zigbee, proprietary), recovery after lost connectivity, sensor drift over time.
Regulatory compliance testing
Regulatory compliance testing produces the evidence package that auditors and regulators actually read. It is not a separate test type so much as a documentation discipline overlaid on every other type above.
What gets produced: traceability matrices linking each requirement to its test case, validation summary reports for HIPAA, audit trail samples for FDA review, accessibility conformance reports for ADA scrutiny, software bill of materials for vulnerability disclosure, predetermined change control plans for any AI-enabled functions.
This is where most healthcare projects discover that the importance of QA testing in healthcare software is not in finding bugs but in proving you tried. Healthcare app testing is seven parallel evidence pipelines, and the cost of merging them late is always higher than the cost of running them in parallel from day one.
Testing AI/ML components in healthcare software
Testing healthcare applications that include AI components now means validating not just code, but model behaviour, training data quality, drift over time, and the change-control plan that governs every retrain.
Why AI/ML in healthcare needs its own testing approach
AI in clinical software has two properties that break traditional QA. Models are probabilistic, so a "passing" test means the confidence score sits in an acceptable range rather than equaling an expected value.
Models also drift: the same model that scored 94% sensitivity in March can drop to 87% by September because the patient population shifted or imaging hardware was upgraded, and neither failure shows up in unit tests.
The FDA's December 2024 final guidance on Predetermined Change Control Plans now requires manufacturers to specify in advance which model modifications are permitted post-market and how each one will be validated, which means healthcare domain testing of AI operates inside a regulatory perimeter that did not exist 18 months ago.
How AI tools help testers (and where they don't)
AI is also reshaping how tests get written, executed, and maintained. AI-augmented testing platforms generate test cases from natural-language requirements, self-heal scripts when UI elements move, prioritize execution by predicted defect risk, and analyze failure logs faster than any human reviewer.
According to Gartner, only one in five organizations had adopted AI-augmented testing tools in early 2025, and that figure "is on track to reach 70% by 2028 , marking a 3.5x growth in just a few years". Where these tools fall short is clinical context: a generator can produce 200 valid scenarios for a billing module overnight, but it cannot tell you whether the model handles a paediatric dosage edge case or whether a SNOMED mapping respects clinical hierarchy.
Healthcare IT testing still needs humans who understand medicine in the loop.
Generating test cases with LLMs
The fastest-moving practical use of AI in healthcare QA is LLM-driven test case generation. Teams feed a model the requirements document, the FHIR resource definitions, and a few seed examples, and the model returns hundreds of structured test cases covering boundary conditions, error states, and clinical edge cases.
We have seen this cut test design time by 60% to 70% on integration projects, particularly for HL7 and FHIR validation work covered in our healthcare interoperability guide . The discipline is everything: LLM-generated tests must be reviewed by a clinical SME before they enter the suite, because a confident-sounding test case with a medically incorrect assumption is worse than no test at all.
Validating AI/ML models
Model validation is its own discipline, distinct from feature testing. The minimum evidence package for a clinical AI model includes accuracy, sensitivity, and specificity measured on a held-out test set; performance breakdowns by demographic subgroup to surface bias; calibration curves showing predicted probabilities match observed outcomes; drift monitoring that triggers retraining when distribution shifts cross a threshold and adversarial robustness tests that probe failure modes.
For high-risk applications like cardiac, oncology, and neurology models, the package expands to include external validation across multiple sites, prospective studies on real clinical workflows, and explainability artifacts that let a clinician understand why the model made a given prediction. None of that is optional under FDA review for higher-risk classifications.
What changes when the AI component is SaMD
Software as a Medical Device classification flips the game. Once an AI component is regulated as SaMD, the testing program has to satisfy the FDA's lifecycle expectations: documented risk classification, validation evidence proportional to risk class, post-market surveillance with active monitoring of model performance, and a change-control plan that pre-defines every permitted model update.
SaMD QA is not a phase that happens before launch but a continuous process running the life of the product, which is why we build this layer into our quality assurance services for AI-enabled clinical products.
Healthcare Software Testing Best Practices
The healthcare software testing market is on track to grow at 13.56% annually through 2031, faster than the global software testing market average. That growth signals one thing for engineering leaders: the bar for what counts as "tested" in a clinical product keeps rising, and the practices that worked five years ago will not pass an FDA review in 2026. Six practices separate the teams that ship cleanly from the teams that learn the hard way.
- Treat the test plan as a regulatory artifact, not an engineering one. Build the test plan from the requirements traceability matrix, not from the sprint backlog. Every test case must trace back to a documented requirement, a regulation, or a clinical safety hazard, and every result must be retrievable for an auditor years after release. If the plan only makes sense to your QA lead, it will not survive an FDA inspection.
- Shift left, but ship the evidence. Run security scans, accessibility checks, and integration tests in CI on every commit, not as pre-release gates. The earlier a defect surfaces, the cheaper it is to fix and the cleaner the audit trail looks. Pair this with automated software testing in healthcare that produces structured evidence outputs, such as JUnit reports tagged with requirement IDs, ready to drop into the validation package.
- Validate AI/ML separately from feature code. AI components need their own pipeline: statistical performance tests across demographic subgroups, drift monitoring, calibration curves, and explainability artifacts attached to every release. Treat the model as a regulated artifact with its own change control plan, not as another feature in the product backlog. Skip this and your post-market surveillance findings become someone else's lawsuit.
- Bring clinical SMEs into the test design phase, not the review phase. A clinician reviewing a finished test suite catches the obvious bugs. A clinician sitting with QA during test design surfaces the dangerous edge cases that QA alone would never imagine: paediatric weight-based dosing, drug-drug interactions across formularies, off-label use patterns. Budget for SME hours upfront, not at the end.
- Build for cross-jurisdictional evidence from day one. If you ship in the U.S. and EU, your test artifacts have to satisfy both HIPAA and GDPR auditors. Tag every test case with the regulations it serves, then generate per-jurisdiction evidence packages on demand. We follow this pattern across our healthcare software development services because retrofitting jurisdictional evidence after launch is one of the most expensive mistakes a healthcare product team can make.
- Test the failure modes, not just the happy path. Healthcare software fails in physical-world ways: dropped Bluetooth connections to glucose monitors, EHR sync failures during shift change, lab results arriving in a corrupted HL7 message. Run chaos engineering against integration boundaries, simulate degraded networks, and validate the system's behavior when downstream services time out. The bugs that hurt patients live in the failure paths, not the happy ones.
What types of healthcare software need testing?
Not all healthcare software carries the same risk, but every category that touches patient data, clinical decisions, or regulated workflows needs structured testing.
As of July 2025, the Bipartisan Policy Center cites the FDA's public database listing over 1,250 AI-enabled medical devices authorized in the U.S., up from 950 a year earlier.
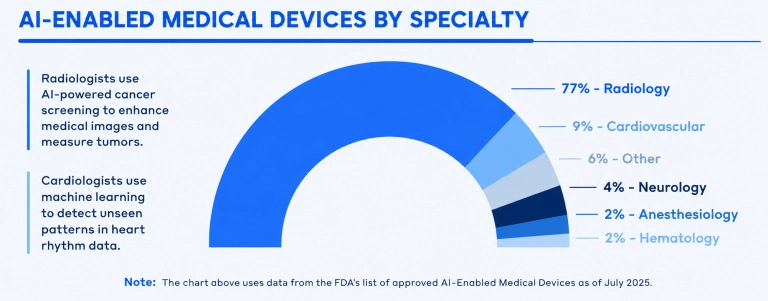
That is just the regulated AI subset. The broader healthcare application testing surface covers seven distinct software categories, each with its own validation profile.
| Category | What It Does | Test Focus | Why It Matters |
| Electronic Health Records (EHR/EMR) | Central source of patient data, integrates with labs, pharmacies, billing, imaging | Data integrity, audit trails, role-based access, HL7/FHIR integration contracts | Corrupts the source of truth every other system depends on |
| Telemedicine and Virtual Care | Real-time video, chat, e-prescribing, EHR sync across mobile and desktop | Video quality under degraded networks, end-to-end encryption, prescription routing, HIPAA session logging | Strands clinicians mid-consultation or exposes PHI through misconfigured streams |
| Medical Device Software | Standalone clinical software and firmware running on physical devices like pumps and pacemakers | Signal accuracy, firmware update verification, wireless protocol resilience, behavior under battery drain | Subject to FDA risk-based oversight and the international standard for medical software lifecycles; high-risk classes need documented evidence for every code branch |
| AI-Powered Clinical Decision Support | Suggests diagnoses, recommends treatments, flags patient deterioration risk | Model accuracy across demographic subgroups, calibration of confidence scores, drift monitoring, explainability artifacts | The recommendation has to be defensible in a malpractice case |
| Patient Engagement and Mobile Health | Patient portals, symptom checkers, medication reminders, chronic disease management | Cross-device compatibility, WCAG accessibility, secure authentication, offline data sync reliability | Reaches patients with limited tech fluency and zero tolerance for friction. We rebuild this layer for clients through our healthcare software development services |
| Healthcare Analytics and Population Health | Ingests EHR, claims, and wearable data to surface trends and risk-stratify populations | ETL pipeline accuracy, query performance against billion-row datasets, statistical validity of risk scores, audit logs for every transformation | Miscalculated risk score at population scale misroutes resources and patients |
| Revenue Cycle and Administrative Software | Billing, claims processing, prior authorization, scheduling | ICD-10 and CPT code mapping, claim validation, denial workflow logic, payer system integration | Bugs delay reimbursement, deny coverage, and quietly damage patient access |
| Healthcare Interoperability and Integration Middleware | Connects EHRs, labs, imaging, billing, devices, and third-party platforms through APIs, HL7, FHIR, and integration layers | API contract testing, FHIR/HL7 mapping accuracy, terminology normalization, consent and access rules, retry logic, error handling | A failed integration can send incomplete, delayed, duplicated, or misrouted data across the entire care ecosystem |
Healthcare software testing team structure
The composition of a healthcare QA team has shifted faster in the last 18 months than in the previous decade. Generative AI is now the top-ranked skill for quality engineers, ahead of core QA fundamentals. For healthcare specifically, that shift adds a new role to the team chart: someone who can validate the AI/ML components that increasingly drive clinical decisions.
The exact lineup varies by project size and budget, but six roles show up in nearly every serious healthcare software testing program:
- QA Manager: owns testing scope, schedule, tooling, and the regulatory evidence pipeline. In healthcare, the role is more about audit defensibility than test execution.
- Test Engineer: designs and executes test cases across functional, integration, and exploratory dimensions. Pairs with clinical SMEs to catch dosing edge cases and malformed HL7 messages before they reach production.
- Test Automation Engineer: builds and maintains automated suites in CI, manages AI-augmented test generation, and integrates output directly into the validation evidence package.
- AI/ML QA Engineer: the newest role on the chart. Validates model accuracy across demographic subgroups, monitors drift, and produces the evidence that satisfies the FDA's Predetermined Change Control Plan requirements. Typically grown from senior test engineers paired with data scientists rather than hired ready-made.
- Compliance Consultant: ensures every test artifact aligns with HIPAA, HITECH, FDA, EU MDR, and country-specific frameworks. Translates between QA leads and regulators, catching documentation gaps engineers do not know are missing.
- Test Lead: owns a specific workstream: writes the plan, runs the schedule, coordinates with development and clinical SMEs.
How Binariks approaches healthcare application testing
Binariks approaches healthcare software testing as part of the engineering workflow, not as a final pre-release checkpoint. For healthcare products, our QA teams help validate the areas where defects create the highest risk: protected health data, clinical workflows, integrations, access controls, audit logs, system performance, and AI-driven behavior.
Depending on the product and regulatory context, our healthcare QA work may include manual and exploratory testing, automated regression testing, API and microservices testing, HL7/FHIR integration testing, security and access-control validation, performance testing, CI/CD-integrated test runs, and documentation that supports client-side compliance and audit preparation.
For AI-enabled healthcare software, testing also needs to go beyond standard functional checks. Binariks can support validation strategies for data quality, model output consistency, edge cases, bias and fairness risks, human-in-the-loop workflows, explainability needs, and model performance monitoring after release.
For example:
AI-powered early heart disease detection solution
Binariks worked on an AI-based healthcare solution designed to support earlier detection of heart disease risk.
For this type of product, testing is not limited to checking whether the application interface works. QA needs to consider the reliability of input data, model behavior across different scenarios, false-positive and false-negative risks, secure handling of sensitive health information, and how results are presented to healthcare users. This is where healthcare domain knowledge, AI validation, and software testing need to work together.
Across all our healthcare projects, the pattern is the same: healthcare software quality has to be built into delivery from the beginning.
When testing covers workflows, integrations, security, data handling, performance, and AI behavior early, teams are better prepared to release safely, support compliance work, and avoid rebuilding evidence under deadline pressure.
FAQ
Author

Share