
The global healthcare interoperability market is set to smash a USD 6.09 billion valuation, growing at a massive 14.9%. It’s a forced upgrade pushed by TEFCA and the CMS Interoperability Rule. Every hour your staff spends playing detective with mismatched medical records is an hour you’re paying for a problem that shouldn't exist.
According to Business Research Insights, a "46% workforce skill gap " is holding things back, but the ones who fix it are winning big.
At Binariks, we see the receipts. Any firm that dodges SMART on FHIR protocols this year is going to get buried under admin work while the competition cruises ahead. This article breaks down the healthcare interoperability challenges wrecking your budget and how to fix them before it's too late.
After reading this article, you will know:
- How to dodge the technical mess that’s currently stalling 30% of health systems
- Why AI-assisted interoperability is the only way to survive data mapping in 2026
- How to use the regulatory landscape to make your legacy vendors actually do their jobs
- The exact steps to set up a system that keeps your data locked down but accessible
Check out this guide and stop letting your data sit in a silo.
What is healthcare interoperability?
So, what is interoperability in healthcare is the difference between a doctor seeing a messy pile of scanned faxes and having a clean timeline of a patient’s health history right on their screen.
We categorize this flow into four distinct layers to make sense of the mess:
- Foundational: The basic "pipes". It’s the ability to move data from point A to point B.
- Structural: The grammar. This ensures the receiving system knows exactly where the patient's name ends and their lab results begin.
- Semantic: The meaning. This is the gold standard where a "heart attack" in one database is recognized as a "myocardial infarction" in another, leaving no room for clinical errors.
- Organizational: The rules of the road. This covers the legal and social framework that lets data cross state lines or different hospital networks securely.
Technological innovation is creating opportunities for stakeholders across segments by automating workflows, promoting data connectivity and interoperability, and generating actionable insights.
At Binariks, we see this transition in real-time. However, ignoring the challenges of interoperability in healthcare, from data silos to regulatory friction, is exactly how "manageable" projects turn into budget-draining nightmares.
Why healthcare interoperability matters in 2026
According to Medical Economics , "The result is that care teams spend valuable time reconciling information that was supposed to be interoperable in the first place".
Cutting the administrative waste
Every time a clinician has to re-order a lab test because the previous results are trapped in a legacy EMR, you are flushing cash. When our team at Binariks develops custom EHR and EMR software , we focus on automating these manual handshakes.
By syncing medical devices directly with the data layer, we've seen providers handle 20% more patient volume without adding a single administrative head. Failing to address the problems with interoperability in healthcare now means you are effectively subsidizing your competitors' agility.
Weaponizing regulatory compliance
With the CMS Interoperability Rule and TEFCA in full swing, being "compliant" means you have the infrastructure to join national networks that others are locked out of. We see many organizations struggle because they treat interoperability challenges in healthcare as a one-time patch. They "wrapper" old systems rather than modernizing the core.
At Binariks, we help clients move past this by implementing SMART on FHIR architectures that satisfy GDPR Article 32 and CMS mandates simultaneously. This transforms a regulatory headache into a verified seal of security and reliability that patients and insurers actually trust.
Radical cooperation across the care continuum
Healthcare in 2026 is a team sport. Whether you are dealing with TPAs, insurers, or specialized labs, your ability to cooperate depends entirely on your API's handshake. Standardized data exchange means mergers and acquisitions don't have to result in two years of "integration hell". It means a patient can walk into a clinic in a different state, and their history is already there, mapped and ready.
We recently proved this by helping a client overcome the "Legacy Tech Anchor" through a comprehensive EHR system modernization . By migrating their outdated infrastructure to a modern, scalable architecture, we eliminated the technical debt that was stifling their growth. It turned their system into a high-speed digital gateway that reduced administrative overhead and improved clinical data accuracy.
Top healthcare interoperability challenges
Whether it's the USD 1 million penalties for "information blocking" or the sheer weight of legacy tech, the challenges of interoperability in healthcare are evolving faster than most providers can patch them.
1. The data silo standoff
Data silos are the ultimate enemy of clinical efficiency. Even in 2026, important patient information often remains trapped in isolated databases, billing, labs, or specialty EHRs, that refuse to talk to each other. According to IBM, "Nearly 77% of respondents agree or strongly agree that data silos hinder the organization's ability to perform real-time analytics and make data-driven decisions”.
When our team at Binariks conducts a thorough software architecture audit , we often find that "integration" is just a thin wrapper over a mess of disconnected tables. Barriers to interoperability in healthcare like these effectively force your high-paid clinicians to act as manual data bridges, wasting hours every week on "swivel-chair" data entry.
2. The information blocking trap
The federal government has lost patience with vendors who charge "gatekeeper" fees or create proprietary APIs to keep data locked in. Under the latest CMS Interoperability Rule, enforcement has entered a new, more aggressive phase.
According to the HIPAA Journal , "A major enforcement initiative was launched in September 2025, targeting noncompliance, which allocated additional resources to support investigations and hold entities accountable for blocking the sharing of electronic health information”.
In early 2026, the Assistant Secretary for Technology Policy (ASTP/ONC) began issuing formal letters of nonconformity to EHR developers, signaling that the era of "wait and see" is over. We help our clients navigate these healthcare data interoperability challenges by building independent, FHIR-compliant layers that bypass vendor lock-in entirely.
This is why we often suggest a bespoke healthcare software development approach. It allows you to own your data endpoints rather than renting them from a vendor whose business model relies on your fragmentation.
3. The "patient matching" identity crisis
One of the most persistent barriers to interoperability in healthcare remains the lack of a universal patient identifier. When data flows between systems, matching "John D. Smith" to "Jon Smith" is more than a technical hurdle, it is a massive financial and clinical risk. Inaccurate patient identification costs the U.S. healthcare system over USD 6.7 billion annually, with individual hospitals losing an average of USD 2.5 million each year due to these errors.
When a specialist cannot be 100% certain that an incoming record belongs to the patient in front of them, they are forced to default to redundant testing to ensure safety. This lack of "identity integrity" is one of the primary healthcare data interoperability challenges that prevents automated systems from scaling.
Without a rock-solid way to verify that data from ten different sources belongs to one single human, "connected" healthcare remains fragmented and dangerously prone to error.
4. The legacy tech anchor
You cannot build a 2026 digital experience on a 1996 foundation. Many health systems are still anchored by legacy platforms that are not equipped to handle modern protocols or real-time data streams.
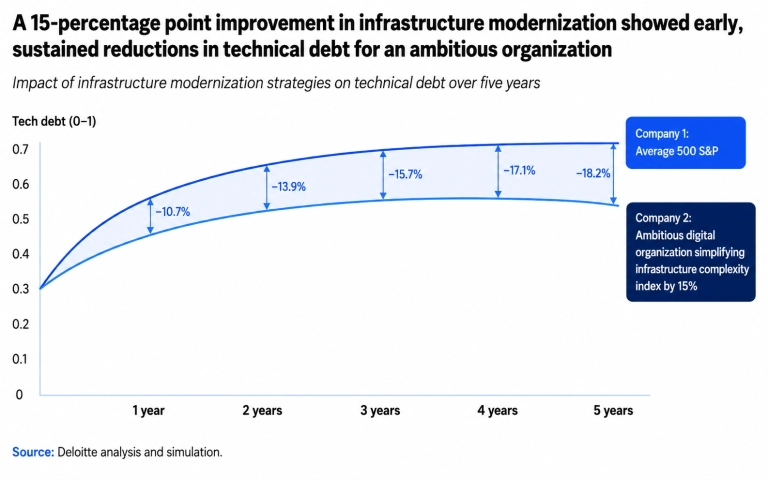
According to Deloitte, "Technical debt accounts for 21% to 40% of an organization's IT spending", a staggering figure that represents value trapped within outdated infrastructure.
Refactoring these systems is expensive, but the "do nothing" strategy is costlier. This burden is one of the most significant issues with interoperability in healthcare, as older integration methods are often slow, costly to maintain, and lack the adaptability required for the latest SMART on FHIR standards.
Organizations that fail to move beyond these aging "monoliths" find themselves unable to participate in the high-speed, data-driven ecosystem that 2026 demands.
5. The cybersecurity surface area
More connections mean more open doors. As we push toward full interoperability, the attack surface for ransomware and data breaches expands exponentially.
Third-party exposures and vulnerable Internet of Medical Things (IoMT) devices are among the top threats in 2026. By moving to a standardized, interoperable framework, you can apply a "Zero Trust" model across all endpoints, making your entire network more resilient than a collection of unpatched silos.
6. The semantic language barrier
Data moves, but meaning gets lost in translation. One system might use ICD-10 codes, while another uses SNOMED CT, and a third uses "free text" notes. 20-40% of critical data points are often missing or inconsistently formatted in typical EHR records.
This semantic gap is the biggest hurdle for AI-assisted interoperability. AI can't generate insights from garbage data.
At Binariks, we focus on semantic normalization, ensuring that a "heart attack" in one database is understood exactly the same way in another. Without this layer of "meaning", your interoperability project is just an expensive way to move noise around.
7. The "connected but not actionable" paradox
A major technical hurdle in 2026 is that data "exchange" does not equal data "usability". While more systems are technically connected than ever before, the information arriving at the point of care often lacks the necessary context to be useful.
Even though interoperability has improved data exchange, data usability remains a critical limitation to scale, impacting the effectiveness of real-time clinical activation and AI initiatives.
This creates a "digital paradox": the more we standardize, the more administrative noise we generate if that data isn't actionable. These challenges with interoperability in healthcare arise when external records sit in separate portals instead of being integrated directly into the clinician's workflow.
At Binariks, we combat this by designing interoperability solutions that focus on "active" integration, filtering and injecting relevant data points directly into the EHR interface so doctors spend time treating patients rather than hunting through fragmented files.
8. The workforce "tech-fatigue" barrier
Interoperability is often treated as a technical problem, but in 2026, it has become a human-centric one. Every poorly integrated tool or fragmented data stream adds to the "cognitive load" of an already exhausted medical workforce.
A 2026 report from Deloitte notes that "health system executives cited workforce challenges as their top concern for 2026, and more than 90% said improving productivity would be a priority". Check this out:
When systems don't talk to each other, the "bridge" is usually a nurse or a doctor doing manual data entry. This is a primary driver of burnout and one of the most stubborn barriers to interoperability in healthcare.
True success requires moving beyond just "connecting pipes" to creating user-centric digital health platforms that remove friction rather than adding it. For instance, in our case study building a comprehensive Medicare data analytics platform, we focused on automating the deduplication and cleansing of records from disparate public and private sources.
By delivering a "single source of truth" directly to clinicians, the system reduced data acquisition time by 50%, ensuring that interoperability actually served the staff instead of becoming another task on their to-do list.
Healthcare interoperability standards you need to know
Without adhering to universally accepted protocols, any attempt to resolve interoperability issues in healthcare results in yet another isolated solution that only adds chaos to the ecosystem.
The foundation of a modern ecosystem
To avoid common interoperability problems in healthcare, the industry has shifted from simple file sharing to the exchange of "meaningful data" using these core standards:
- HL7 FHIR (Fast Healthcare Interoperability Resources): This is the "gold standard" for modern data exchange. FHIR uses RESTful APIs, allowing developers to create modular applications that plug into any EHR seamlessly. Our experts have analyzed this protocol in depth, covering the benefits of the FHIR standard as well as the comprehensive FHIR implementation process.
- SMART on FHIR: A framework that allows third-party applications to run securely inside an EHR without complex custom coding. It is critical for solving healthcare interoperability problems related to the gap between clinical data and analytical tools. For more, see our dedicated guide on SMART on FHIR application development.
- TEFCA (Trusted Exchange Framework and Common Agreement): This is the U.S. national "roadmap" defining the rules for data exchange between different networks. TEFCA creates a unified infrastructure where every participant can rely on the security and legitimacy of transactions.
- IHE Profiles: These specifications define exactly how to use existing standards (HL7, DICOM) to solve specific clinical scenarios, such as transferring medical imaging results (MRI/CT).
- CMS Interoperability Rule: Not just a standard, but a regulatory mandate requiring payers and providers to give patients access to their data via APIs. Ignoring this rule in 2026 is a direct path to heavy fines and lost market trust.
If your organization is navigating a system expansion or seeking to modernize its core infrastructure, adopting FHIR best practices is the most effective way to ensure your digital foundation is scalable and secure from day one.
By prioritizing structured data mappings and secure API gateways, you can transform interoperability from a regulatory hurdle into a long-term competitive advantage.
What does FHIR integration look like in 2026?
By 2026, the conversation has shifted from "can we connect?" to "how fast can we activate the data?" The convergence of FHIR R4/R5 and the TEFCA framework has created a standardized "interstate highway system" for medical records. Integrating via FHIR today isn't just about moving a PDF; it’s about granular, real-time access to specific resources without the bloat of an entire legacy record.
This combination of TEFCA + FHIR represents the largest leap in interoperability in a decade. It replaces the "one-to-one" custom integrations of the past with a "one-to-many" model, where once you are on the network, you can securely shake hands with any other participant.
Detailed FHIR R4 API integration workflow
Modern integration follows a highly structured, automated path. Instead of manual data dumps, 2026 workflows utilize SMART on FHIR to ensure that security and data mapping happen in milliseconds.
| Phase | Technical Description | Real-World Outcome |
| Secure Identity Verification | The requesting application introduces itself to the hospital's data server using modern security protocols. It requests specific permission to see only the data it needs (like vitals) rather than the patient's entire history. | Secure, "least-privilege" access. This ensures high-level privacy compliance and prevents unauthorized data exposure. |
| Capability Statement Discovery | Before sending data, the two systems perform an automated check-in. The requesting app asks the server, "What can you provide?" The server responds with a list of available data types and the specific ways it can send them. | This prevents technical "translation errors". It ensures both systems are perfectly aligned on the technical language they will speak before the transfer begins. |
| Targeted Data Retrieval | Instead of downloading a massive, 50-page clinical summary, the app sends a precise request for a specific data point, such as a heart rate from a specific date or a specific allergy record. | Drastic reduction in digital "noise". Clinicians get the exact answer they need instantly without digging through irrelevant documents. |
| Language and Meaning Translation | The incoming data is passed through a terminology engine. This service translates local, non-standard medical codes from the source facility into globally recognized medical languages like SNOMED or LOINC. | Guarantees "semantic interoperability". A diagnosis recorded in a rural clinic is correctly understood and categorized by a specialist's system in a major city. |
| Direct Workflow Injection | The newly translated data is embedded directly into the doctor's current screen within their EHR. It can even trigger automated "alerts" (like a drug-allergy warning) based on the fresh information. | The external data appears as if it were native to the EHR. No separate logins, no portal-hopping, and no manual data entry for the medical staff. |
The real power of FHIR lies in its ability to support computable data. Because information is structured as discrete, individual resources, AI models and automated systems can consume it instantly to provide predictive analytics or decision support at the point of care. This shifts the focus from simply "moving files" to ensuring those files have immediate clinical utility.
Successfully navigating this transition requires more than just a technical switch; it demands a comprehensive FHIR implementation plan that aligns your business goals with the latest regulatory standards. By building an architecture where semantic meaning is preserved at every hop, you turn a simple digital connection into a powerful diagnostic tool that saves time and lives.
AI-assisted interoperability: The next frontier
By 2026, the industry has realized that while standards like FHIR provide the "pipes", the data flowing through them is often still messy, inconsistent, and unstructured. This is where AI-assisted interoperability has become the critical operating layer. AI is no longer a futuristic experiment; it is the engine performing the "heavy lifting" of data normalization and clinical reasoning that humans simply cannot do at scale.
AI solves the most stubborn healthcare interoperability problems by acting as an intelligent translator. Instead of manual mapping, machine learning models now automate:
- Semantic normalization: AI can ingest "free text" clinical notes or non-standard local codes and automatically map them to standardized terminologies like SNOMED CT or LOINC with over 90% accuracy.
- Intelligent patient matching: Using probabilistic algorithms, AI reduces the "identity crisis" by identifying duplicate records across different systems even when names or addresses are formatted differently.
- Predictive data cleansing: AI tools profile and remediate clinical data in real-time, identifying anomalies or missing values before they reach the clinician's dashboard.
Infrastructure still rules
It is vital to understand that AI is not a magic wand that resolves interoperability issues in healthcare in a vacuum. AI cannot generate reliable insights from "garbage" data without a standardized foundation. To be effective, AI requires a standardized infrastructure to access clean, structured datasets.
Without the "technical scaffolding" of APIs and common data models, AI remains trapped in silos, unable to perform the cross-system reasoning required for modern care.
The real frontier in 2026 isn't just "having AI", but having an AI-ready data strategy that leverages FHIR-based architectures to turn fragmented information into a unified, intelligent clinical asset.
How to overcome healthcare interoperability challenges
Navigating the healthcare interoperability landscape in 2026 requires more than a “plug-and-play” mindset. To turn interoperability challenges into operational and clinical advantages, healthcare organizations need to move beyond reactive fixes and adopt a proactive, architecture-first strategy.
Here is a practical roadmap for addressing some of the most persistent interoperability issues in healthcare.
1. Adopt a FHIR-first or FHIR-facade data architecture
The shift from document-heavy exchange to resource-based access is becoming increasingly important for modern healthcare systems. By implementing a FHIR-native layer or a FHIR facade over legacy systems, organizations can reduce dependence on proprietary interfaces and make clinical data easier to access, exchange, and reuse.
This approach supports more granular data access, allowing applications to query specific clinical resources without overloading the broader system. It can also help organizations modernize legacy environments gradually, without requiring a disruptive rip-and-replace transformation.
2. Implement semantic normalization and terminology governance
Technical connectivity alone does not solve interoperability. Healthcare systems also need to understand data in the same way.
Terminology services, governed mappings, and standardized vocabularies such as LOINC, SNOMED CT, ICD-10, RxNorm, and local code systems can help normalize data from different sources. Instead of relying on manual interpretation, organizations can create structured mapping workflows that improve consistency, reduce ambiguity, and support safer clinical data exchange.
However, semantic normalization should include validation, exception handling, and clinical oversight, especially when data is used for care decisions, analytics, or automation.
3. Prioritize zero-trust security principles
As healthcare data exchange expands across systems, partners, applications, and devices, the security model must evolve as well. A zero-trust approach helps organizations avoid relying on implicit trust based on network location alone.
In practice, this means stronger identity and access management, least-privilege permissions, continuous monitoring, encryption, audit trails, and consistent security policies across APIs and connected systems. Standardized APIs can support this model, but they still need to be implemented within a broader security architecture and governance framework.
4. Use AI-assisted data mapping carefully
Manual-only data mapping is difficult to scale across complex healthcare environments. AI-assisted tools can help accelerate data extraction, mapping recommendations, terminology matching, and transformation of unstructured content such as forms, PDFs, or clinical notes.
At the same time, AI should be treated as an accelerator, not a replacement for governance. Clinical data mapping still requires validation, traceability, human review for high-risk cases, and clear rules for handling uncertain or low-confidence outputs.
Used responsibly, AI-assisted mapping can reduce repetitive manual work and help teams move faster while maintaining control over data quality.
5. Build for clinical workflow, not just technical compliance
Effective interoperability should reduce friction for clinicians, not create another portal or workflow burden. Instead of forcing users to search across multiple systems, organizations can use standards-based integrations to surface relevant data, alerts, and decision support inside existing clinical workflows.
Approaches such as SMART on FHIR applications, CDS Hooks, and EHR-integrated data exchange can help make interoperability more useful at the point of care. The goal is not just to connect systems, but to deliver the right information at the right time in a way that supports clinical efficiency.
How Binariks can help
Healthcare interoperability projects require a combination of software engineering, data architecture, healthcare domain knowledge, and security-aware delivery. Binariks helps healthcare organizations design and implement integration architectures that support scalable, secure, and standards-aligned data exchange.
Our teams support clients with:
- Regulatory and standards alignment: Helping design systems with applicable interoperability, privacy, and security requirements in mind, including CMS, ONC, HIPAA, and FHIR-related implementation needs.
- Legacy infrastructure modernization: Building middleware, FHIR facades, integration layers, and modernization roadmaps that help connect older systems without unnecessary disruption.
- Healthcare data engineering: Designing secure data pipelines, terminology mapping workflows, and integration architectures that improve data quality and prepare healthcare organizations for analytics and AI-enabled use cases.
- Workflow-oriented interoperability: Creating integrations that support clinicians and operations teams by reducing duplicate work, improving data availability, and fitting into existing care delivery processes.
At Binariks, we help healthcare organizations move from fragmented systems toward more connected, secure, and scalable digital ecosystems. Our healthcare software development teams bring engineering expertise, interoperability experience, and domain understanding to complex healthcare technology initiatives.
Explore our healthcare case studies to see how we have helped clients address interoperability, modernization, and healthcare software development challenges, or contact us to discuss a custom roadmap for your organization.
Author

Share